Minimal Change Disease
Contents
What is Minimal Change Disease?
Minimal Change Disease (MCD for short) is a kidney disease in which large amounts of protein is lost in the urine. It is one of the most common causes of the Nephrotic Syndrome (see below) worldwide. The kidneys normally work to clean the blood of the natural waste products that build up over time. To do this they have to filter all of the blood in the body many times each day. That is in fact what urine is- filtered blood. Normally, the kidneys can filter this blood without losing any of the proteins that are supposed to remain in circulation. When the kidney filters are damaged, however, protein sometimes “slips through” into the urine. This is called proteinuria.
Although Minimal Change Disease can be suspected from many of its different symptoms (see below), the only way to be certain of the diagnosis is with a biopsy.
What does it look like?
First, a quick overview of the kidney- most people have two kidneys, one on each side of their lower back. All of the blood in your body passes through your kidneys many times during the day, and each time blood goes through some of it gets filtered by the glomeruli (singular = glomerulus). This filtering is how your body cleans the blood (and removes extra water), and some of the filtered blood becomes your urine. Urine isn’t red (like blood) because the red blood cells, which give blood its color, are too big to fit through the filters. A glomerulus is just a tiny bag of blood vessels through which blood gets filtered, and all of the filtered out blood (urine) runs into tubes (ureters) that eventually lead to your bladder.
In MCD, the biopsied glomeruli look normal under a “light microscope,” which can magnify objects to hundreds of times their normal size. This is where the disease gets its name, Minimal Change- it describes the lack of differences seen under a standard microscope. It is not until the glomeruli are seen under an “electron microscope”, which can magnify an object to over a million times its normal size, that the characteristic changes of MCD can be seen.
|
|
|
|---|
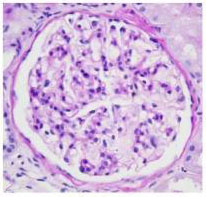
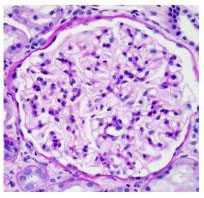
Above are shown two glomeruli, shown as they look under a light (standard) microscope. Notice how similar the two specimens are.
|
|
|---|

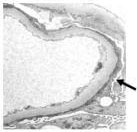
Above are two more glomeruli, this time as seen under an electron microscope. Again, the normal kidney specimen is on the left. Notice the four black arrows in the normal specimen. They are pointing out a normal feature of kidney cells called “foot processes”. These foot processes are an important part of the kidney filters themselves, and are essential for determining what gets filtered out of and what stays in the circulation.
Now look at the picture of the kidney filter from a patient with Minimal Change Disease (on the right). The individual foot processes can no longer be made out- it is like they have all just “melted” together into a single thin layer. This important barrier in the filtration process can no longer keep protein from being filtered out of the blood and into the urine.



How did I get it?
The short answer is that no one is sure. Minimal Change Disease is one of the most common causes of the Nephrotic Syndrome however, especially in children. In fact, almost 90% of children 10 and under with the Nephrotic Syndrome end up having MCD when biopsied (as opposed to 20% of adults).
Doctors tend to put MCD in two categories, primary and secondary. Primary means that the disease occurs on its own, for no obvious reasons. This is by far the most common type. Secondary means that we think the MCD was caused by, or is at least associated with, another medical condition. MCD has been associated with all of the following, usually in adults:
| Drugs | NSAIDs, lithium, some antibiotics, bisphophonates |
|---|---|
| Malignancy | Leukemia, Lymphoma |
| Infection | Syphillis, HIV, Hepatitis |
| Allergy | Associated with multiple environmental allergies |
Again though, secondary MCD is very uncommon, and a diagnosis of MCD does not confer any risk of having (or prompt a “workup” for) any of the above conditions.
What are the symptoms?
The most noticeable symptom of MCD is often edema, or swelling, which can be profound. This typically starts in the feet and legs, but can move into the hips and abdomen as well. In contrast to many of the other diseases that can cause the Nephrotic Syndrome, the proteinura and edema of MCD can develop very rapidly- almost overnight. Other symptoms include high blood pressure, high cholesterol, and a tendency to form blood clots. Unlike the majority of other kidney diseases, especially those that cause the Nephrotic Syndrome, the ability of the kidney to clean the blood is often unaffected in MCD. This is especially true in children and young adults.
None of the above symptoms, or even all of them together, is specific for MCD. If you or your doctor are concerned about MCD, the only way to know for sure is to have a kidney biopsy. However, because of how common this disease is in children, when a child is diagnosed with the Nephrotic Syndrome he is typically treated for Minimal Change Disease before undergoing a biopsy. If this therapy does not immediately improve symptoms and decrease the amount of protein in his urine, then a biopsy to look for another cause is considered.
The Nephrotic Syndrome
When someone has a great deal of protein in their urine, they can often develop what is called the “Nephrotic Syndrome.” This syndrome always includes-
- >3 g proteinuria (protein in the urine) per day
- Hypoalbuminemia (less protein in the blood than normal)
- Peripheral edema (swelling)
It often also includes- - Hyperlipidemia (high cholesterol)
- Hypercoagulability (increased tendency to form blood clots)
What is the treatment?
Minimal Change Disease is one of the more treatable kidney diseases, especially in children. Therapy almost always consists of a course of oral steroids (prednisone), which is generally effective within weeks. A complete remission is not uncommon, though the disease can come back later in life. Patients with recurrent MCD, or with MCD that does not completely resolve with steroids, may require other forms of chemotherapy.
It is also important for someone with MCD to be on medication that reduces the amount of protein in the urine. These medications are called ACE-inhibitors (angiotensin converting enzyme inhibitors) and ARBs (angiotensin II receptor blockers). If urine protein levels are high, the complications of the Nephrotic Syndrome should also be considered; patients should receive routine cholesterol screening/treatment, and their physicians should always remember their tendency to form clots. Finally, every patient with MCD must have their kidney function monitored regularly. If kidney function declines, certain other interventions may become necessary.
What is the prognosis?
Even in adults, Minimal Change Disease typically has a favorable prognosis. Over 90% of patients will respond to oral steroids, with most of these having a complete remission. However, more than 50% of the adults who go into remission will relapse at some point in their lives, and for these patients either another course of steroids or another form of chemotherapy entirely may be necessary.
Although it is rare for Minimal Change Disease itself to lead to End Stage Kidney Disease, some patients with MCD eventually develop another disease called Focal Segmental Glomerulosclerosis (FSGS). FSGS is generally seen as a more aggressive disease, with less treatment options and more of a tendency towards eventual kidney failure.
Minimal Change Disease Podcast
This UNC Kidney Center podcast features Dr. Ron Falk discussing Minimal Change Disease with a parent of a child who has the disease. He answers questions such as “What causes Minimal Change Disease?” and “What steps can I take to ensure optimal health?”